Liver Hemangioma
What’s wrong with my liver?
Hemangioma:
This is a patient information booklet providing specific practical information about hepatic hemangioma in brief. Its aim is to provide the patient & his or her family with useful information on this particular liver problem, the procedures and tests you may need to undergo, treatment approaches, risks involved, duration, expenses and helpful advice on coping successfully with the problem. If you require more information, Dr. D.R.Kulkarni or your doctor will be able to provide more information.
What Is Liver?
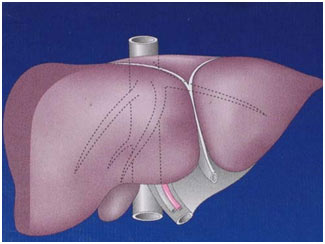
The human liver is a reddish brown organ normally weighing approximately 1.5% of body weight. It is the largest internal organ. It is located in the right upper part of the abdominal cavity, resting just below the diaphragm under the protection of rib cage. Liver is broadly divided into a large right and a relatively small left lobe. Additionally there is a small lobe called caudate lobe. The right and left lobes are further subdivided into segments. These subdivisions help in planning liver surgery when a patient needs removal of a portion of liver.

Apart from a patch where it connects to the diaphragm the liver is covered entirely by peritoneum, a thin, double-layered me mbrane that reduces friction against other organs. The peritoneum folds back on itself to form the falciform ligament and the right and left triangula r ligaments. These “ligaments” are in no way related to the true anatomic ligaments in joints, and have essentially no functional importance. An exception to this is the falciform ligament, which attaches the liver to the anterior body wall from within.
Liver is supplied by two large blood vessels, one called the hepatic artery and one called the portal vein. The hepatic artery carries blood from the aorta, whereas the portal vein carries blood containing digested nutrients from the entire gastrointestinal tract and also from the spleen and pancreas. The hepatic portal vein supplies approximately 75% of the liver’s blood supply, the hepatic artery accounting for the remainder of its blood flow. Oxygen is provided from both sources.
Before entering the liver the portal vein and hepatic artery divide into right and left branch for each of the lobes. They further subdivide within the liver tissue to supply each segment in total 9 in number. Blood flows through channels called sinusoids and empties into the central vein of each lobule. (Each lobule is made up of millions of hepatic cells, which are the basic metabolic cells.). The central veins coalesce into hepatic veins, which leave the liver. There are 3 main hepatic veins that drain blood from liver into a large vein (inferior vena cava), which carries blood from lower portion of body to heart. Apart from the 3 main Hepatic Veins there are many smaller draining veins, which enlarge if any or all of the 3 veins are blocked due to diseases like cirrhosis or hepatic vein thrombosis or veno-occlusive disorders.
The caudate lobe is a separate structure, which receives blood flow from both the right- and left-sided vascular branches and then drains through small veins directly into the vena cava.
The bile produced in the liver is collected in bile canaliculi, which merge to form bile ducts. Bile ducts are tube like structures carrying bile produced within liver to the intestine. Within the liver, these ducts are called intrahepatic (within the liver) bile ducts, and once they exit the liver they are considered extrahepatic (outside the liver). The intrahepatic ducts eventually drain into the right and left hepatic ducts, which merge to form the common hepatic duct. The term biliary tree is derived from the arboreal branches of the bile ducts. The cystic duct draining the gallbladder joins with the common hepatic duct to form the common bile duct. Bile can either drain directly into the duodenum via the common bile duct, or be temporarily stored in the gallbladder via the cystic duct. The common bile duct and the pancreatic duct enter the second part of the duodenum together at the ampulla of Vater.
The liver has a “capsule” around it, which contains nerve endings, accounting for pain when the liver enlarges and stretches its capsule. The damaged liver has an amazing ability to regenerate itself. The body needs only about 20% of the liver to live, and if a piece is cut out or injured, it can grow back. Sometimes, however, the liver gets chronic diseases, which impair its ability to regenerate. It can become infiltrated with fat (“steatosis”), shrink from chronic alcohol or viral exposure (“cirrhosis”) or grow large from infection or a blocked blood drainage (“hepatomegly”). Any inflammation of the liver, whether caused by germs, drugs, or radiation, is called hepatitis. A damaged liver may heal, or may slowly fail and require liver transplant to save the patient’s life.
What Is The Function Of Liver?
The liver is an astounding laboratory sustaining metabolism. Liver’s main job is to filter the blood coming from the digestive tract, before passing it to the rest of the body. The liver detoxifies chemicals and metabolizes drugs. As it does so, the liver also secretes bile that ends up back in the intestines. Bile contains bile salts, which are responsible for digestion and absorption of food material. The liver is responsible for carbohydrate, fats & protein metabolism and also makes albumin, proteins important for blood clotting and other functions. It also produces various clotting factors, stores glucose, fats, vitamins like A, D3, B12 & minerals like iron & copper. This myriad of functions makes clear why the liver is essential to life.
What Are The Tests To Check Liver Function?
The diagnosis of liver function is made by blood tests. Liver function tests can readily pinpoint the extent of liver damage. Usually in liver diseases patient can have a combination of raised bilirubin, increase in liver enzymes, drop in blood albumin levels, alteration in clotting test results, depending on the type of liver disease.
If liver function is altered then other tests are asked depending on clinical picture and lab results. If hepatitis is suspected, then tests to detect cause of hepatitis are done. Sometimes, one may require an ultrasound or a CT scan or MRI to produce images of the liver and diagnose liver tumors, abscess, and other pathologies.
Physical examination of the liver is not accurate in determining the extent of liver damage. It can only reveal presence of tenderness or the size of liver, but in most cases, some type of radiological study is required to examine it. In patients with chronic liver disease noninvasive tests like Phytate liver scan (nuclear scan) and Ultrasound elastography of liver (Fibroscan) are done to assess the liver status.
However, the ideal way to determine damage to the liver is with a biopsy. A biopsy is not required in all cases, but may be necessary when the cause or extent of damage is unknown. A needle is inserted into the skin just below the rib cage and a biopsy is obtained. The tissue is sent to the laboratory, where it is analyzed under a microscope. Sometimes, a radiologist may assist the physician performing a liver biopsy by providing ultrasound guidance.
What Is Hemangioma?
A hemangioma is a noncancerous tumor made of widened (dilated) blood vessels that are atypical or irregular in arrangement and size. These vascular spaces may contain thrombin, calcifications, or prominent scarring (sclerosed
hemangioma). Phleboliths are rare. Grossly, these lesions often appear as having a flat surface or as bulging subcapsular lesions. Lesions are reddishblue and well demarcated from surrounding tissue. Large tumors may become pedunculated.
How Common Is Liver Hemangioma?
Hemangioma is the most common benign tumor affecting the liver. The widespread use of noninvasive abdominal imaging modalities has led to increased detection of it even when it is asymptomatic.
What Is A Giant Hemangioma?
Giant hemangiomas are large hemangiomas and the size definition actually varies in the books but commonly anything more than 5cms is considered giant hemngioma.
What Causes A Hemangioma In Liver?
It’s not clear what causes a liver hemangioma to form. It is probably congenital — meaning that you’re born with it. It is certainly not familial or genetically inherited. Some associations are observed regarding occurrence and growth of a hemangioma like age, sex, hormonal influence, drugs etcetera.
Women, especially with a history of multiparity, are affected more often than men. Women who have been pregnant are more likely to be diagnosed with a liver hemangioma than women who have never been pregnant. Women who used hormone replacement therapy for menopausal symptoms may be more likely to be diagnosed with liver hemangioma than women who did not.
Several pharmacologic agents have been postulated to promote its growth. Steroid therapy , estrogen therapy, and pregnancy can increase the size of an already existing hemangioma.
Hepatic hemangiomas can occur at all ages. Most hepatic hemangiomas are diagnosed in individuals aged 30-50 years. Female patients often present at a younger age and with larger tumors. Hepatic hemangiomas may be seen in
infancy. They have also been detected prenatally in a growing fetus. Babies may develop a type of hepatic hemangioma called benign infantile hemangioendothelioma. This rare, noncancerous tumor has been linked to high rates of heart failure and death in infants. Infants are usually diagnosed by the time they are 6 months old. Hepatic hemangiomas may be seen in 5-10% of children aged 1 year. They typically regress during childhood.
Why Is It Necessary To Investigate a Patient with Hemangioma Of Liver?
Hemangiomas can be mistaken for hypervascular malignancies of the liver or vice versa and can coexist with (and occasionally mimic) other benign and malignant hepatic lesions, including focal nodular hyperplasia, hepatic adenoma, hepatic cysts, hemangioendothelioma, hepatic metastasis, and primary hepatocellular carcinoma.
Additionally liver hemangioma could be one feature of a larger disease complex or a welldefined clinical syndrome. In Klippel-TrenaunayWeber syndrome, hepatic hemangiomas occur in association with congenital hemiatrophy and
nevus flammeus, with or without hemimeganencephaly. In Kasabach-Merritt syndrome, giant hepatic hemangiomas are associated with thrombocytopenia and intravascular coagulation. Osler-Rendu-Weber disease is characterized by numerous small hemangiomas of the face, nares, lips, tongue, oral mucosa, gastrointestinal tract, and liver. Von
Hippel-Lindau disease is marked by cerebellar and retinal angiomas, with lesions also in the liver and pancreas.
Multiple hepatic hemangiomas have been reported in patients with systemic lupus erythematosus.
What are The Symptoms and Signs?
Hemangiomas of the liver are usually small and hence asymptomatic. However, even large hemangiomas remain asymptomatic most often. Most cases of liver hemangioma are discovered during a test or procedure for some other
condition. Most people who have a liver hemangioma never experience symptoms, never show signs and most hemangiomas don’t grow even over long periods or have complications and hence may never need treatment.
But in a small number of people, liver hemangioma will grow, may cause symptoms or complications and require treatment. It’s not clear why this happens. Larger, especially more than 10cms and multiple lesions may produce
symptoms.
Dull pain, vague discomfort, which cannot be explained in words or fullness in the right upper abdomen, is the most common complaint especially when it is located in the right lobe of liver. Hepatic hemangiomas are more common in
the right lobe of the liver than in the left lobe.
Early satiety (feeling full after eating even small amount of food), nausea, and vomiting may occur when large lesions compress the stomach, producing obstruction. This is more common with lesions located in the left side or those
hanging form liver like bunch of grapes.
Rarely, hemangiomas may present as a large abdominal mass. Other atypical presentations include jaundice from compression of the bile ducts, gastrointestinal bleeding, fever of unknown origin or cardiac failure.
In some cases, acute abdominal pain occurs due to various complications like clot formation inside the hemangioma (called thrombosis), hemorrhage into the lesion or free intraabdominal cavity, twisting or torsion if there is a stalk for hanging hemangioma or compression of adjacent tissues or organs.
Consumption of coagulation factors causes an illness that resembles a systematic inflammatory process with findings of fever, weight loss, anemia, thrombocytosis, increased fibrinogen level, and elevated erythrocyte sedimentation
rate.
Babies with benign infantile hemangioendothelioma may have a growth in the abdomen, failure to survive or grow, anemia, and heart failure The only findings upon physical examination are, infrequently, an enlarged liver, a palpable abdominal mass or the presence of an arterial bruit over the right upper quadrant.
Can It Cause Cancer?
It may be unsettling to know you have a mass in your liver, even if it’s a benign mass. However, there’s no evidence that an untreated liver hemangioma can lead to liver cancer.
Problem comes when one cannot differentiate between a hemangioma from a cancer.
It is usually solitary, but 10% patients can have multiple hemangiomas in their liver.
Will There Be Complications If Left Untreated?
Complications are rare with hemangiomas even when they are large in size. They include rupture with resultant hemoperitoneum, intratumoral bleeding, compression of bile ducts and nearby arteries and veins, gastric compression, bleeding inside the bile ducts & heart failure.
Complications depend on the size and location of the tumor.
Women who have been diagnosed with liver hemangioma face a risk of complications if they become pregnant. The female hormone estrogen, which increases during pregnancy, is believed to cause some liver hemangiomas to grow larger. A growing hemangioma can cause signs and symptoms and may require treatment. Having a liver hemangioma doesn’t mean you can’t become pregnant. However, discussing the possible complications with your doctor can help you make a more informed choice.
Medications that affect hormone levels in your body, such as birth control pills, could cause complications if you have been diagnosed with liver hemangioma. But this is controversial. If you’re considering this type of medication,
discuss the benefits and risks with your doctor.
How Is a Patient With Hemangioma of Liver Investigated?
Most patients with liver hemangioma come with the diagnosis on a routine ultrasonography as said before & rarely other form of imaging like CT or MRI. Rarely a diagnosis is made before investiagations because the tumor is large.
The modalities used to aid in the diagnosis of hepatic hemangiomas include ultrasonography, dynamic contrast-enhanced computed tomography (CT) scanning, nuclear medicine studies using technetium-99m (99m Tc) – labeled
RBCs, magnetic resonance imaging (MRI), hepatic arteriography, and digital subtraction angiography.
Ultrasonography is the most commonly used initial diagnostic tool. Serial ultrasonographic examinations are done to monitor any increase in size of the hemangioma over time. Microbubble contrast -enhanced ultrasonography helps in differentiating from a hepatocellular cancer. However, difficulty occurs in large lesions where central thrombosis or scarring may be present. Unfortunately, contrast-enhanced ultrasonography is available at relatively few medical centers.
The finding on ultrasonography of a suspected hemangioma should be diagnostically correlated with CT scan or MRI to ensure a correct diagnosis.
Dynamic contrast-enhanced CT scanning is preferred to routine CT scanning. When requesting a CT scan to investigate a liver mass, the hepatobiliary specialist insists on nonenhanced, arterial, portal venous, and delayed
imaging (the so-called triple phase CT with delayed imaging).
First, the liver is imaged by CT before the administration of intravenous contrast. The next series of images is obtained about 30 seconds after the injection of contrast, at the time that contrast is entering the liver via the hepatic artery. Portal venous imaging occurs 60 seconds later, as contrast is returning to the liver from the
mesenteric veins via the portal vein. Finally, delayed images are obtained several minutes later. If you have already done a CT scan but it is suboptimal & improperly done it is advisable to repeat it properly or do an MRI with proper
technique.
MRI is highly sensitive and specific in the diagnosis of & differentiating liver tumors especially hepatic hemangioma. When gadolinium is used as an intravenous contrast agent, hemangiomas enhance in a fashion similar to that seen on dynamic CT. The sensitivity for detection of hepatic hemangioma is upwards of 90%. Therefore often patient has to go through these 3 forms of imaging sequentially. In spite of all this diagnosis may still be unsure especially
since it is matter of differentiating a benign lesion from a malignant tumor.
Scintigraphic studies using Tc-99m pertechnetate-labeled red blood cells were used for many years to help in diagnosing hepatic hemangiomas. Single-photon emission computerized tomography (SPECT) using Tc99m
pertechnetate-labeled RBCs is more accurate. However, it is not available at all medical centers and with availability of CT & MRI these are now used very infrequently.
Will I Require an Angiography?
The diagnostic accuracy of noninvasive tests has obviated the need for hepatic arteriography also in most cases. However, this invasive modality still may be useful in helping to diagnose some hepatic hemangiomas.
Is It Possible To Diagnose a Small Hemangioma Convincingly?
Diagnostic accuracy diminishes for all imaging modalities when assessing a liver lesion that is less than 2 cm in diameter. MRI is the most accurate radiologic study to establish the diagnosis of a small hepatic tumor.
MRI used to confirm the diagnosis when a probable hemangioma is detected on ultrasonography. Nuclear medicine studies will be used when nature of a lesion when the diagnosis is equivocal on CT or MRI.
Will I Require a Biopsy?
Percutaneous biopsy is frequently used for liver tumors whose pathology cannot be established on CT scan or MRI. But biopsy of a suspected hepatic hemangioma carries an increased risk of hemorrhage. Liver biopsy is not done in most circumstances where a hemangioma is high in the differential diagnosis of a hepatic mass. Liver biopsy is only used when radiologic study results and alpha-fetoprotein testing are equivocal.
Will There Be More Tests?
Tumor markers like Alpha-FetoProtein (AFP), CA 19-9, and CarcinoEmbryonicAntigen (CEA) are done and normal levels bolster clinical suspicion of a benign hepatic mass.
Blood investigations like CBC or LFT are not done routinely as they do not contribute to diagnosis and are required only if a surgery is planned.
Do All Liver Hemangiomas Require Treatment?
Most hepatic hemangiomas are small and asymptomatic at the time of diagnosis, and they are likely to remain that way. In addition, malignant transformation has not been reported in hepatic hemangiomas. Even large hemangiomas have very little risk of complications. For these reasons, most asymptomatic hepatic hemangiomas are left safely alone.
How Is The Patient Followed Up?
Once the diagnosis of hepatic hemangioma is confirmed by radiologic studies, there will not be any further follow up if it is a small hemangioma. If there is any doubt about diagnosis you will be asked to follow up after I month again to repeat the investigations.
For larger hemangioma you will be advised to undergo ultrasonography at 6 months and at 12 months after the initial diagnosis. Providing that no change in hemangioma size has occurred, long-term follow-up radiologic studies are probably not necessary. However if you continue to do USG every 6 months and follow up with your surgeon it is always better.
Certainly, patients with a new onset of abdominal pain deserve a follow-up imaging study. The same is true for patients who are undergoing treatment with estrogens or have become pregnant. Finally, patients with large
hemangiomas (i.e., >10 cm) may deserve long-term follow-up radiologic studies, perhaps annually, because of their probable increased risk of complications however it is not mandatory.
Is There Any Nonsurgical Therapy Available?
Until recently, no medical therapy capable of convincingly & permanently reducing the size of hepatic hemangiomas has been described. Modalities like radiation or drugs like thalidomide are used occasionally with unconvincing effect.
When Does A Patient With Liver Hemangioma Warrant Surgery?
Hepatic hemangiomas warrant therapy only if they are causing significant symptoms and the cause of pain is proved to be hemangioma beyond doubt. Therefore all tests must be performed to rule out other causes for pain like peptic ulcer disease, colitis, gastroduodenitis, gallstones & irritable bowel syndrome. Upper GI endoscopy, colonoscopy, imaging studies should be performed to rule out other causes. Unfortunately, in some individuals, determining
if the symptoms are caused by a hemangioma or by another process (e.g., irritable bowel syndrome) is difficult.
Surgical treatment may be appropriate in cases of rapidly growing tumors. Surgery may also be warranted in cases where a hepatic hemangioma cannot be differentiated from hepatic malignancy on imaging studies. Obviously for patients coming with hemangioma complications surgery is mandatory.
So Size Of Hemangioma Does Not Matter?
Size actually does not matter in most cases and as said above it is the symptoms that decide the requirement of treatment. The management of very large (>10 cm) hepatic hemangioma is controversial. Resection is advocated for such lesions because of the potential risk of complications.
What Is The Nature Of Surgery?
Surgical resection and surgical enucleation are the treatments of choice. In resection, a hemangioma-containing portion of liver with surrounding normal liver tissue is removed. In enucleation, hemangioma is removed without
removing any of the surrounding liver tissue.
The size and location of a lesion will influence the surgeon’s decision to perform either a formal segmental resection of the hemangioma or an enucleation of the hemangioma. Typically, these procedures are performed using an open
approach, but laparoscopic surgery can be performed in some cases. Hepatic lobectomy may be necessary in the case of large lesions. Very rarely (large and / or multiple lesions) liver may have to be replaced (transplantation).
In general, both surgical resection and enucleation are safe and are well tolerated by patients. Typically, postoperative complications are less and the average length of hospital stay is 6 days. Surgery is technically more demanding in resection.
Will It Recur After Surgery?
In the absence of tumor-promoting factors, such as estrogen therapy, hemangiomas rarely recur after successful resection.
What Is Done If Hemangioma Ruptures?
Spontaneously ruptured hemangioma is an emergency life-threatening situation. These patients are usually admitted with acute abdominal pain & shock state. Patients are immediately taken to ICU and top priority will be
given to hemodynamic stabilization. Patient will require various accesses for rapid fluid and blood transfusion (called central or jugular or subclavian or femoral line). Patient may require support for breathing too (ventilator). After patient is stabilized investigations are done to find the cause of shock including USG & CT scan, which confirm that patients critical condition is due to a ruptured hemangioma.
The patient will be then immediately shifted to radiology department where interventional radiologist does an urgent Arterial embolization. Branches of the hepatic artery feeding the hemangioma are embolized with polyvinyl alcohol, metal coils and other substances. Embolization results in stopping the bleeding. It also shrinks the tumor, thereby minimizing the risk of complications. Patient may get pain & fever after this procedure.
If this facility is not available then patient will certainly require a surgery with due risk to life. During surgery, resection or enucleation is usually not attempted unless patient is stable since there is risk of more bleeding and usually a surgical ligation of the hepatic artery is performed. Selective ligation of large feeding vessels used to be performed in the days when embolization was not available or is not available. It has the same effect like embolization provided all feeders are ligated, but this is difficult and therefore results are not assured. Once the patient is stabilized, formal surgical resection of the hepatic hemangioma can be performed.
Are There Alternative Treatments If I Don’t Want Surgery Or I Am Unfit?
Surgical resection may not be possible in certain cases because of the massive or diffuse nature of the lesion, its proximity to vascular structures, or the patient’s comorbidities. Minimally invasive therapies for hepatic hemangioma include arterial embolization, radiofrequency ablation, and hepatic irradiation can be tried in such patients. However the long-term success rate of embolization (without subsequent surgical resection) is not known. Percutaneous radiofrequency ablation may be used to improve abdominal pain in patient with symptomatic hepatic hemangiomas. But this would be useful only in small tumor which otherwise also do not need therapy. Hepatic irradiation over several weeks may cause tumor regression and symptom relief with minimal morbidity but no assurance.
What Is The Treatment In Infants?
Treatment for infantile hemangioendothelioma depends on the child’s growth and development. The following treatments may be needed:
- Embolization
- Tying off (ligation) a liver artery
- Medications for heart failure
- Surgery to remove the tumor
In infants whose tumor is only in one lobe of the liver, surgery is a cure, even if the child has heart failure.
Are There Any Dietary & Physical Activity Restrictions?
No special dietary management is required. Also no restriction of physical activity is indicated for most patients with hepatic hemangiomas. Patients with large hemangiomas may need to be instructed to avoid trauma to the right upper abdominal quadrant.
Is There Any Medical Management?
No medications are useful to shrink or eradicate hepatic hemangiomas.
What Is The Prognosis?
Overall, a patient with a hepatic hemangioma has an excellent prognosis. Malignant transformation has not been described.
Above information will help you to make an informed decision but it cannot replace the professional advice and expertise of a doctor who is familiar with your condition. You may have questions that are not covered; you should discuss these with your surgeon. You must remember every individual is different.
Doctors Dealing With Liver Disease That You May Meet
Endoscopist: This may be a gastroenterologist or a surgeon who is able to undertake endoscopy (examination of the stomach or bowel using a flexible telescope). A few endoscopists can also perform ERCP and EUS, which are special forms of endoscopy that examine the biliary and pancreatic ducts and the pancreas.
Gastroenterologist: A physician who is highly specialized in ‘gut’ problems.
General physician: A consultant medical doctor who works in a hospital and who is broadly specialized including ‘gut’ problems.
General surgeon: A consultant surgeon who works in a hospital and who is broadly specialized including ‘gut’ problems.
HepatoPancreatoBiliary surgeon: A surgeon who is highly specialized in pancreato-biliary & liver operations.
Glossary
MRI – Magnetic Resonance Imaging :
A type of scanning performed to diagnose problems not picked up by regular investigations.
CT SCAN – Computerized Tomography:
A type of scanning performed to diagnose problems not picked up by regular investigations.
ERCP – Endoscopic Retrograde Cholangiography:
An endoscopic procedure performed to visualize bile & pancreatic ducts & treat the disease endoscopically whenever possible.
EUS – Endoscopic UltraSound:
An endoscopic procedure performed to visualize pancreas & biliary tract from very close, diagnose problems, obtain biopsies and at times treat the disease too.
MRCP – Magnetic Resonance Cholangio Pancreatography
Leave a Reply