Liver Abscess Treatment & Management
This is a patient information booklet providing specific practical information about liver abscess in brief. Its aim is to provide the patient & his or her family with useful information on this particular liver problem, the procedures and tests you may need to undergo, treatment approaches, risks involved, duration, expenses and helpful advice on coping successfully with the problem. If you require more information, Dr. D.R. Kulkarni or your doctor will be able to provide more information.
What Is Liver?
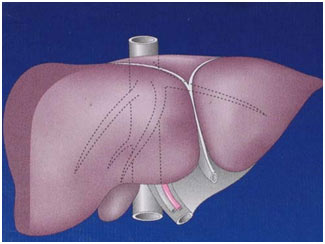
The human liver is a reddish brown organ normally weighing approximately 1.5% of body weight. It is the largest internal organ. It is located in the right upper part of the abdominal cavity, resting just below the diaphragm under the protection of rib cage. Liver is broadly divided into a large right and a
relatively small left lobe. Additionally there is a small lobe called caudate lobe. The right and left lobes are further subdivided into segments. These subdivisions help in planning liver surgery when a patient needs removal of a portion of liver.
 peritoneum, a thin, double-layered membrane that reduces friction against other organs. The peritoneum folds back on itself to form the falciform ligament and the right and left triangular ligaments. These “ligaments” are in no way related to the true anatomic ligaments in joints, and have essentially no functional importance. An exception to this is the falciform ligament, which attaches the liver to the anterior body wall from within.
peritoneum, a thin, double-layered membrane that reduces friction against other organs. The peritoneum folds back on itself to form the falciform ligament and the right and left triangular ligaments. These “ligaments” are in no way related to the true anatomic ligaments in joints, and have essentially no functional importance. An exception to this is the falciform ligament, which attaches the liver to the anterior body wall from within.
Liver is supplied by two large blood vessels, one called the hepatic artery and one called the portal vein. The hepatic artery carries blood from the aorta, whereas the portal vein carries blood containing digested nutrients from the entire gastrointestinal tract and also from the spleen and pancreas. The hepatic portal vein supplies approximately 75% of the liver’s blood supply, the hepatic artery accounting for the remainder of its blood flow. Oxygen is provided from both sources.
Before entering the liver the portal vein and hepatic artery divide into right and left branch for each of the lobes. They further subdivide within the liver tissue to supply each segment in total 9 in number. Blood flows through channels called sinusoids and empties into the central vein of each lobule. (Each lobule is made up of millions of hepatic cells, which are the basic metabolic cells.). The central veins coalesce into hepatic veins, which leave the liver. There are 3 main hepatic veins that drain blood from liver into a large vein (inferior vena cava), which carries blood from lower portion of body to heart. Apart from the 3 main Hepatic Veins there are many smaller draining veins, which enlarge if any or all of the 3 veins are blocked due to diseases like cirrhosis or hepatic vein thrombosis or venoocclusive disorders.
The caudate lobe is a separate structure, which receives blood flow from both the right- and leftsided vascular branches and then drains through small veins directly into the vena cava.
The bile produced in the liver is collected in bile canaliculi, which merge to form bile ducts. Bile ducts are tube like structures carrying bile produced within liver to the intestine. Within the liver, these ducts are called intrahepatic (within the liver) bile ducts, and once they exit the liver they are considered extrahepatic (outside the liver). The intrahepatic ducts eventually drain into the right and left hepatic ducts, which merge to form the common hepatic duct. The term biliary tree is derived from the arboreal branches of the bile ducts. The cystic duct draining the gallbladder joins with the common hepatic duct to form the common bile duct. Bile can either drain directly into the duodenum via the common bile duct, or be temporarily stored in the gallbladder via the cystic duct. The common bile duct and the pancreatic duct enter the second part of the duodenum together at the ampulla of Vater.
The liver has a “capsule” around it, which contains nerve endings, accounting for pain when the liver enlarges and stretches its capsule. The damaged liver has an amazing ability to regenerate itself. The body needs only about 20% of the liver to live, and if a piece is cut out or injured, it can grow back. Sometimes, however, the liver gets chronic diseases, which impair its ability to regenerate. It can become infiltrated with fat (“steatosis”), shrink from chronic alcohol or viral exposure (“cirrhosis”) or grow large from infection or a blocked blood drainage (“hepatomegly”). Any inflammation of the liver, whether caused by germs, drugs, or radiation, is called hepatitis. A damaged liver may heal, or may slowly fail and require liver transplant to save the patient’s life.
What Is The Function Of Liver?
The liver is an astounding laboratory sustaining metabolism. Liver’s main job is to filter the blood coming from the digestive tract, before passing it to the rest of the body. The liver detoxifies chemicals and metabolizes drugs. As it does so, the liver also secretes bile that ends up back in the intestines. Bile contains bile salts, which are responsible for digestion and absorption of food material. The liver is responsible for carbohydrate, fats & protein metabolism and also makes albumin, proteins important for blood clotting and other functions. It also produces various clotting factors, stores glucose, fats, vitamins like A, D3, B12 & minerals like iron & copper. This myriad of functions makes clear why the liver is essential to life.
What Are The Tests To Check Liver Function?
The diagnosis of liver function is made by blood tests. Liver function tests can readily pinpoint the extent of liver damage. Usually in liver diseases patient can have a combination of raised bilirubin, increase in liver enzymes, drop in blood albumin levels, alteration in clotting test results, depending on the type of liver disease.
If liver function is altered then other tests are asked depending on clinical picture and lab results. If hepatitis is suspected, then tests to detect cause of hepatitis are done. Sometimes, one may require an ultrasound or a CT scan or MRI to produce images of the liver and diagnose liver tumors, abscess, and other pathologies.
Physical examination of the liver is not accurate in determining the extent of liver damage. It can only reveal presence of tenderness or the size of liver, but in most cases, some type of radiological study is required to examine it. In patients with chronic liver disease noninvasive tests like Phytate liver scan (nuclear scan) and Ultrasound elastography of liver (Fibroscan) are done to assess the liver status.
However, the ideal way to determine damage to the liver is with a biopsy. A biopsy is not required in all cases, but may be necessary when the cause or extent of damage is unknown. A needle is inserted into the skin just below the rib cage and a biopsy is obtained. The tissue is sent to the laboratory, where it is analyzed under a microscope. Sometimes, a radiologist may assist the physician performing a liver biopsy by providing ultrasound guidance.
What Is a Liver Abscess?
Liver abscess is a pus-filled cavity in the liver.
what causes a liver abscess?
Liver abscess is caused by bacterial or parasitic infection. Very rarely fungi cause them. Bacterial liver abscess is called pyogenic liver abscess. Parasites called amoeba, which cause the intestinal disorder amebic dysentery, cause amebic liver abscess.
what is the source for bacterial infection?
Bacterial infection can spread to liver from
- Bile ducts containing tubes/stent or when they get blocked by stones, tumors etcetera,
- abdomen when there is appendicitis, enteritis, colitis, diverticulitis (outpunching from intestine most commonly large intestine), or perforated bowel. Infection reaches liver via the portal venous blood that drains the intestines into liver.
- distant organs like heart valves (endocarditis), kidney (pyelonephritis), lungs etcetera via bloodstream.
what is the source for amoebic infection?
Amebic liver abscess is caused by Entamoeba histolytica, the same organism that causes amebiasis, an intestinal infection also called amebic dysentery. The organism is carried by the blood from the intestines to the liver. The disease spreads through ingestion of amebic cysts in food or water contaminated with feces. The infection occurs worldwide, but is most common in tropical areas where crowded living conditions and poor sanitation exist. Africa, Latin America, Southeast Asia, and India have significant health problems associated with this disease.
what are the other causes?
Liver abscess may result from diagnostic procedures in the liver like Endoscopy of the bile-draining tubes, as well as accidental or surgical trauma to liver.
how do organisms cause abscess?
A liver abscess occurs when bacteria or protozoa destroy hepatic tissue, producing a cavity, which fills with infectious organisms, dead liver cells, and leukocytes. Necrotic tissue then walls off the cavity from the rest of the liver.
what increases risk for a liver abscess formation?
A number of factors increase the risk of developing liver abscess. Not all people with risk factors will get liver abscess. Current, primary abdominal or gastrointestinal infection or a recent endoscopy of the bile-draining tubes increases risk of pyogenic abscess.
Advanced age, alcoholism or heavy alcohol ingestion, compromised immune system due to such conditions as HIV/AIDS or other immunodeficiency, taking corticosteroids, organ transplant, or cancer and cancer treatment, poor nutritional status, travel to regions where amebic infections are common; these factors increase risk of amoebic liver abscess. Avoiding contaminated food or water is the best way to avoid amoebic infections.
what are the symptoms of a liver abscess?
Symptoms of liver abscess vary among individuals & include abdominal pain (especially in the upper right portion of the abdomen), pale stools, dark urine, diarrhea, fever or chills, joint pain, loss of appetite, malaise or lethargy, nausea with or without vomiting , sweating, unexplained weight loss, yellowing of the skin and whites of the eyes (jaundice).
Serious symptoms that might indicate a lifethreatening condition include change in mental status or sudden behavior change, such as confusion, delirium, lethargy, hallucinations and delusions, high fever (higher than 101 degrees Fahrenheit), breathing problems, such as shortness of breath, inability to breathe, wheezing, or choking.
A liver abscess can become dangerous if it opens and spreads the infection. This can happen suddenly, so you should consult your health care provider if you have any of the complaints mentioned above.
Patient usually has fever & racing pulse. Blood pressure is normal or low. Abdomen is tender especially the right side of abdomen, quite often even the right chest is also tender. If there is a rupture of liver abscess the entire abdomen is tight and distended. Patient is unable to pass gas in such a situation because patient has peritonitis. Usually patient has jaundice.
what investigations are done if liver abscess is suspected?
Blood investigations done by your physician will include Complete blood count (CBC), Liver Function Tests. CBC may show high white blood cells, high or normal platelet count unless patients is having underlying chronic liver disease due to alcohol or other cause when platelets are often low.
Liver function tests show elevated bilirubin and elevated liver enzyme levels like SGOT, SGPT, ALKP, and GGTP. Albumin is often low because of infection and liver disease, clotting parameters like prothrombin time & INR are elevated.
how is the liver abscess diagnosis confirmed?
Abdominal ultrasound (USG) is the 1st imaging study asked and usually gives the diagnosis. Rarely it may not show the abscess. Abdominal & pelvic CT scan or MRI will be done to get valuable information regarding source, exact location in the liver, and possibility of complication & hence help in management.
will there be more tests?
Blood is sent for amoebic serology & culture sensitivity for bacteria & stool is tested for amebiasis and sometimes stool culture is done.
Percutaneous needle aspiration of the abscess is sometimes performed to identify the causative organism Aspiration is not performed in all cases. It is done only if abscess is likely to rupture or patient is not responding to regular antibiotics and a culture is required. It is done under USG or CT scan guidance.
how is a liver abscess treated?
When detected in time, liver abscess is usually treatable and often can be cured with a course of antibiotics, antiamoebic agent or a combination of drugs and an abscess drainage procedure.
In case of uncomplicated bacterial liver abscesses intravenous drug therapy needs to be continued for a period of 2 weeks in most circumstances. Initially broad-spectrum antibiotics are used. When the causative organisms are identified, the antibiotic regimen is modified to match the patient’s sensitivities. I.V. antibiotics are administered for minimum14 days and then replaced with oral preparations to complete a 6-week course. Patients who present with various serious complications may require long ICU care followed by ward care, which could stretch, to few weeks.
Left untreated, however, a liver abscess can burst and spread the infection, leading to sepsis, a lifethreatening bacterial blood infection. This then may require a laparoscopic or open surgery to wash out the pus from abdominal cavity & clear the abscess cavity in liver thoroughly. This is done only as a lifesaving measure because patient is very critical when they undergo such surgery and have a high chance long postoperative stay in the ICU and hospital or even a death early or late in the course of disease in spite of all the efforts.
This is especially true for patients who are elderly, diabetic and immune compromised.
Lot of medicines are available for amoebic infection. But some of them work only on the organism in the intestinal lumen, while others will work on the organism in the lumen as well as when it is extraintestinal. A medicine called metronidazole (Flagyl) is the usual treatment for liver abscess. The common problem with these drugs is they cause lot of bitter taste (metallic) in the mouth, nausea and vomiting thereby making it difficult for patients to tolerate in the ideal recommended dosage.
A medication such as iodoquinol is often prescribed by some practitioners to get rid of all the amebae in the intestine, to prevent the disease from coming back. However it must be told here that iodoquinol has serious side effects because of which it should be avoided and if taken should be under strict medical observation. Other safer medications (diloxanide) are available to take care of the cysts of amoeba and should be taken after the abscess has been treated. to prevent recurrence of the abscess.
Sometimes amoebic liver abscesses are infected with bacteria also and it is extremely difficult to differentiate between the two. These patients are treated like pyogenic liver abscess only. In rare cases, the abscess may need to be drained to help relieve complaints.
how is a liver abscess drained nonsurgically?
It is necessary in many cases to drain the abscess since patient is not responding to medical treatment or there is risk of rupture. This is done with a needle or small tube inserted through the abdomen. This surgical procedure is called percutaneous aspiration or percutaneous drainage.
who requires a surgery?
Surgery may be performed to drain pus in unstable patients with continued sepsis (despite attempted non surgical treatment) and for patients with persistent fevers (lasting longer than 2 weeks) after percutaneous drainage and appropriate antibiotic therapy. Surgery is reserved for bowel perforation and rupture into the pericardium.
what are the potential complications of a liver abscess?
Complications of untreated or poorly controlled liver abscess can be serious, even life threatening in some cases. You can help minimize your risk of serious complications by following the treatment plan that you and your health care professional design specifically for you. Complications of liver abscess occur from rupture and include:
- Empyema (pus accumulation in the chest)
- Endocarditis (inflammation of the heart lining and heart valves)
- Liver failure
- Pleural effusion (accumulation of fluid around the lungs)
- Sepsis (life-threatening blood infection)
what is the prognosis?
This condition can be life threatening some patients. The risk for death is higher in people who have many liver abscesses.
how to prevent liver abscess formation?
Where poor sanitation exists, drink purified water and do not eat uncooked vegetables or unpeeled fruit.
Above information will help you to make an informed decision but it cannot replace the professional advice and expertise of a doctor who is familiar with your condition. You may have questions that are not covered; you should discuss these with your surgeon. You must remember every individual is different.
doctors dealing with liver disease that you may meet
Endoscopist: This may be a gastroenterologist or a surgeon who is able to undertake endoscopy (examination of the stomach or bowel using a flexible telescope). A few endoscopists can also perform ERCP and EUS, which are special forms of endoscopy that examine the biliary and pancreatic ducts and the pancreas
Gastroenterologist: A physician who is highly specialized in ‘gut’ problems.
General physician: A consultant medical doctor who works in a hospital and who is broadly specialized including ‘gut’ problems.
General surgeon: A consultant surgeon who works in a hospital and who is broadly specialized including ‘gut’ problems.
HepatoPancreatoBiliary surgeon: A surgeon who is highly specialized in pancreato-biliary & liver operations.
glossary:
MRI – Magnetic Resonance Imaging
A type of scanning performed to diagnose problems not picked up by regular investigations
CT SCAN – Computerized Tomography
A type of scanning performed to diagnose problems not picked up by regular investigations
ERCP – Endoscopic Retrograde Cholangiography.
An endoscopic procedure performed to visualize bile & pancreatic ducts & treat the disease endoscopically whenever possible
EUS – Endoscopic UltraSound.
An endoscopic procedure performed to visualize pancreas & biliary tract from very close, diagnose problems, obtain biopsies and at times treat the disease too.
MRCP – Magnetic Resonance Cholangio- Pancreatography
Leave a Reply