Gall Bladder Cancer
This is a patient information booklet providing specific practical information about gall bladder cancer in brief. Its aim is to provide the patient & his or her family with useful information on this particular gall bladder problem, the procedures and tests you may need to undergo, treatment approaches, risks involved, duration, expenses and helpful advice on coping successfully with the problem. If you require more information, Dr. D.R.Kulkarni or your doctor will be able to provide for more information.
What Is Gall Bladder?
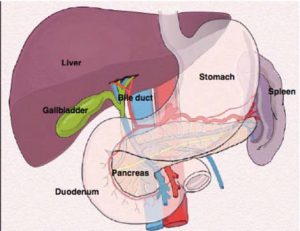
Gall is an old-fashioned word for what we now call bile. The gallbladder is a small sac that lies beneath the liver in the right upper abdomen under the rib cage. It is joined to the bile duct, a tube that comes from the liver and carries bile to the intestine. Bile is a yellow-green viscous fluid helpful in digesting food is produced in liver.
What Is The Function Of Gall Bladder?
The gallbladder stores bile that is produced by the liver and removes water and salt from it. It contracts when we eat, especially fatty food and pushes bile down the bile duct into the intestine.
Is Gall Bladder Necessary For Digestion / Good Health?
The gallbladder is not necessary to maintain good health. After the gallbladder is removed, bile duct increases in diameter slightly and bile flows directly from the liver to the intestines, and digestion proceeds normally.
What Is Cancer?
Cancer can arise in any part of the body when particular cells begin to multiply more than normally and spread into other tissues. Cancer arises because of defects within the genes of cancer cells, although the reason for these defects arising in the first place is not known in most cases. If left untreated, cancers cause harmful effects by invading vital tissues.
How Is Cancer Treated?
Many cancers can be cured by surgery, which is called ‘curative surgery’. In some cases, even though the cancer cannot be removed or can be removed only partly, surgery is still very helpful in relieving symptoms, in which case it is called ‘palliative surgery’. Even if a patient has had ‘curative surgery’ the cancer cells may have already spread in blood vessels to other organs but cannot be seen or felt or diagnosed by investigations. Because of this it is often necessary to recommend additional treatment after curative surgery in the form of chemotherapy (giving drugs which kill cancer cells). This type of additional treatment is called ‘adjuvant therapy’ and helps to increase the chances of being cured properly. If the cancer cannot be removed by surgery it is often useful to give chemotherapy, radiotherapy or a combination of these to slow down the growth of the cancer. This type of treatment is known as ‘palliative therapy’. There have been big advances in the use of chemotherapy and radiotherapy so that many of the serious side effects that used to be seen with these treatments do not occur frequently. The use of chemotherapy and radiotherapy for many cancers is being improved all the time by asking patients to participate in ‘clinical trials’. This means that the doctor treating the patient is not sure which type of treatment is best and so will allocate one or other treatment with the patient’s permission. Inevitably some patients will die from cancer. It is important from the outset that the patient and relatives are both aware of what the situation is and are encouraged to talk freely about this between themselves and with friends. Most patients will be able to lead a normal life right up to the last few days or weeks. Pain and vomiting is a feature of some cancers but there are now very effective drugs to deal with both. No patient should suffer from unbearable pain. Hospices are specialized hospitals dealing with the needs of patients with advanced cancer. Patients may be attached to a hospice as an outpatient as well as being an inpatient. The most important doctor coordinating cancer care will be the General Practitioner. Many patients choose to spend their last days at home. In some cases, depending on the home circumstances and the patient’s particular problem, this is not possible so the hospice or even the hospital may be the best place. It is always important to be open about the problem. Doctors involved with patients and their relatives will always be keen to discuss the issues and answer all their questions. Remember that even if it is not possible to guarantee a cure, treatment can prolong life and give patients an excellent quality of life. Also, remember that cancer can be cured!
What Is Gall Bladder Cancer?
Gallbladder cancer is cancer that begins in the gallbladder. It is uncommon in most parts of the world but not in India. Here it is fairly common especially in the northern parts of India & the Gangetic belt. When gallbladder cancer is discovered at its earliest stages, the chance for a cure is very good. But most gallbladder cancers are discovered at not so early or late stage, when prognosis is often very poor. Gallbladder cancer is difficult to diagnose because it often causes no signs or symptoms. Also, the relatively hidden nature of the gallbladder makes it easier for gallbladder cancer to grow without being detected.
What Are Causes & Risk Factors?
It’s not clear what causes gallbladder cancer. Doctors know that gallbladder cancer forms when healthy gallbladder cells develop changes in their genes (mutation). These mutations cause cells to grow out of control and to continue living when other cells would normally die. The accumulating cells form a tumor that can grow beyond the gallbladder and spread to other areas of the body. Most gallbladder cancer begins in the cells that line the inner surface of the gallbladder. Gallbladder cancer that begins in this type of cell is most commonly called adenocarcinoma. This term refers to the way the cancer cells appear when examined under a microscope. Gallbladder cancer is more common in women than it is in men & your risk of gallbladder cancer increases as you age. There are a number of risk factors that may increase your chances of developing this type of cancer. These include:
Gall stones and inflammation
Gall bladder cancer is more likely to occur in people who have a history of gallstones or in people who have inflammation of the gall bladder for a long period( chronic cholecystitis). However, most people who have gallstones or an inflamed gall bladder won’t develop gall bladder cancer.
Polyps
These are non-cancerous (benign) tumours of the gall bladder that may carry risk of developing gall bladder cancer. Only 5% of polyps are actually cancerous. These are adenomas and rarely adenomyoma. Polyps more than 1 cm in size have a higher risk of having malignancy.
Abnormal bile ducts
Gall bladder cancer is slightly more common in people who are born with (congenital) abnormalities of the bile ducts like cystic change or abnormal connection with pancreatic duct.
Porcelain gall bladder
People who have a condition called porcelain gall bladder, in which calcium forms in the wall of the gall bladder, also have a slightly increased risk of this type of cancer.
Obesity
Being overweight increases your risk of developing gall bladder cancer.
What Are Types Of Gall Bladder Cancers?
Most cancers of the gall bladder are a type of cancer called adenocarcinoma. They start in the lining of the gall bladder. It’s very rare in people under 50 and is most often seen in people over the age of 70. But in India it is seen frequently in young and middle aged patients too especially in women with gall stones from northern states like UP, Bihar, West Bengal and even northeastern states. It’s more common in women than men.
There are many other rare types of gall bladder cancers.
What Are The Signs And Symptoms?
Early gall bladder cancer most often causes no symptoms and is usually discovered unexpectedly when someone has surgery to remove gallstones. About 1 in 5 gall bladder cancers are found in this way.
Most tumors are only discovered at an advanced stage when they have already spread. They can cause a variety of symptoms, including sickness, fever, weight loss without effort, loss of appetite, nausea and pain in the tummy (abdomen).
If the cancer spreads to & blocks the bile duct, it may stop the flow of bile from the gall bladder into the small bowel. This causes jaundice, dark urine and pale stools. The skin may become itchy.
These symptoms may be caused by other problems, such as gallstones or infection of the gall bladder or cancer of bile duct, but it’s important to get them checked by your doctor.
How It Is Diagnosed?
Usually you begin by seeing your family physician for one or more of the complaints mentioned. He/she will examine you & will conduct baseline blood tests like blood count, bilirubin, liver enzymes and USG. When there is suspicion of a gall bladder pathology/ cancer, then they will refer you to a specialist for further investigations that may be necessary and for expert advice and treatment.
Your lab studies may show a normal or high leucocyte count, anemia, jaundice, poor liver function and nutrition. When you are suspected to have a gall bladder cancer you are advised various abdominal imaging studies including CT scan, MRI scan, tests to examine the bile ducts like ERCP (endoscopic retrograde cholangio- pancreatography) , MRCP, PTC.
When cancer is suspected blood is checked for tumor marker substance like CA 19.9. If it is significantly elevated it points towards the gall bladder cancer. However it has limitations in interpretations in that it can rise even in noncancerous biliary obstructions.
Will I Require A Biopsy?
A biopsy is usually advised in most situations to confirm a cancer. However, it should be avoided when a gall bladder cancer is suspected and is possible to be cured by surgery. A biopsy is likely to spread the cancer, hence it is avoided in most situautions where there is a possibility of surgical cure. If chemotherapy is to be given prior to surgery or as the only treatment then biopsy is mandatory.
What Is The Treatment Of Gall Bladder Cancer?
The treatment of gall bladder cancer is difficult because of late diagnosis and advanced stage of disease at the time of diagnosis since the disease easily involves surrounding organs and important indispensable arteries and veins. The best treatment for gall bladder cancer is surgery to remove the cancer (resection) by a specialist hepatobiliary surgeon. However this is possible only when the cancer is not spread to other tissues like liver, peritoneum, lungs, and bone etcetera.
Not all patients are lucky enough to undergo a curative surgery for various reasons and these patients undergo various palliative therapies. (Treatments that palliate or reduce complaints but don’t cure the patient)
What Is Staging Of Cancer?
Staging is to determine to best of one’s ability how far a cancer has or has not spread from the organ of origin to the surrounding tissues, important blood vessels & other important structures; nearby & distant lymph glands & distant organs.
Cancer can spread in the body, either in the bloodstream or through the lymphatic system. The lymphatic system is part of the body’s defence against infection and disease. The system is made up of a network of lymph glands that are linked by fine tubes (lymph vessels). Doctors will usually look at the nearby lymph nodes to find the stage of the cancer.
In the early stage of any cancer the disease is limited to the affected organ and has not gone beyond the walls or tissue of that particular organ. In this stage the disease can be removed completely and cured. In the next stage the disease has spread to the surrounding lymph glands or surrounding adjacent organs. In this stage also the cancer can be removed completely but a much larger extent of removal is required and more organs and lymph glands need to be removed. More structures need to be repaired or reconstructed & this increases chances of postoperative complications and a slightly higher chance of postoperative death. Patients in this stage would also have inferior survival and higher chance of cancer recurrence and hence would need postoperative chemo or radiotherapy.
In the advanced stage the cancer spreads to the distant lymph glands like in the chest and neck or distant organs like liver lung brain bone etcetera. These patients cannot be cured by surgery or any other means and only a palliative treatment with chemotherapy or radiotherapy or other therapies specific to that cancer are used. A lot of these patients are unfit for any form of therapy and are given only supportive or symptom specific treatment. Some of the advanced stage patients are enrolled in various trials for cancer chemotherapy.
In short, cancers that are not spread beyond organ of origin are usually curable, those spread to nearby tissues & lymph glands are locally spread & will require radical surgery followed by additional treatment & when cancer spreads to distant organs surgery is not possible & therapy is palliative.
Knowing the particular type and the stage of the cancer helps the doctors to decide on the most appropriate treatment and also explain the chances of cure & life expectancy ( PROGNOSIS).
How Is Staging Done?
This requires the use of a special CT scan. The specialist may request this investigation even if this has already been performed by the referring hospital. Another ‘staging’ procedure is to perform laparoscopy and/or laparoscopic ultra- sound. This is a short operation under general anesthetic. Using ‘key hole’ surgery a telescope is inserted into the abdomen to examine the organs. A special ultrasound ‘probe’ may be used to look at deeper tissues. Some centers may also use a PET scan. This is pretreatment staging. In operated patients final staging is after the surgery when specimen is examined by the histopathologist.
What Is Grading?
Grading refers to the appearance of the cancer cells under the microscope and gives an idea of how quickly the cancer may develop. Low-grade means that the cancer cells look very like normal cells; they are usually slow growing and they are less likely to spread. In high-grade tumours the cells look very abnormal, are likely to grow more quickly and are more likely to spread.
Will I Withstand A Major Surgery?
It is necessary to ensure that you are fit enough to survive the major surgery. In order to determine this there will be some extra investigations.
An ECG (electro-cardio-gram) records the electrical heart activity and may be done on the ward or in the cardiology (meaning heart) department. A cardiac echo (doctors say echocardiogram or just echo) uses ultrasound waves to look at how the chambers of the heart are working. An echo is performed either in the cardiology department or the X-ray department. In selected cases you may be asked to undertake some exercise on a treadmill before and after the ECG or the echo.
PFTs (or pulmonary function tests) look at how well your lungs are functioning. This is usually performed in a special department and involves breathing into a tube attached to a machine.
After these tests a specialist anesthetist, who will tell you what the risks are of undergoing the surgery, will examine you. In addition, a heart specialist may assess you.
Only patients with good cardiac, lung and renal function are suggested major surgeries. Other patients may also undergo a major surgery but with added risk. Patients with highly compromised organ functions are advised against a surgery and sent for other treatment options.
What Is The Nature Of Surgery?
If you have very early gall bladder cancer restricted to only the innermost linings of the gall bladder wall, a simple cholecystectomy would suffice. Obviously this information cannot be gathered with currently available investigations in the preoperative period, hence this is usually an afterthought in patients who are incidentally found to have a cancer in their gall bladder specimen after cholecystectomy. These are very fortunate patients and do not need any more treatment.
However as the cancer starts breaching the deeper layers of gallbladder wall more radical surgery is required. This is a major operation that removes the gall bladder, the surrounding tissues, lymph glands and sometimes parts of other organs like liver, bile duct, pancreas & intestine that may be affected by cancer. Depending on this extent of removal they are called radical cholecystectomy with or without hepatectomy with or without pancreaticoduodenectomy (whipple’s procedure). Sometimes nearby major arteries and veins are removed and reconstructed too. Whether surgery is possible or not depends on the results of the investigations described above.
How Long Will The Operation Go On?
These are complex operations and would last from 3 hours for a relatively less radical operation to 10 hours for a very radical extensive operation involving multiorgan resection.
How Long Will The Patient Stay In The Hospital?
After the surgery patient is shifted to ICU for further management and stabilization. This takes 48-72 hours and then patient is shifted to room. In more complex operations or if there are complications patients may stay in ICU for longer time.
Usually surgery involving removal of only gall bladder with surrounding lymph glands and sliver of liver tissue will involve hospital stay of 7 days. But as the surgery becomes more radical, involves removal of bile duct with reconstruction, removal of major portions of liver, pancreas, intestines etcetera, stay is prolonged to 2-3 weeks and at times more if there are minor or major complications.
Does Surgery Involve Complications?
These operation for advanced gall bladder cancer involving removal of portion of liver or bile duct or pancreas or reconstruction of vessels are complex, have their own sets of minor and major complications. The chance of a minor complication following a major surgery for gall bladder cancer is 15%, that of a major complication is 5% and the risk of death is 2-5%.
The minor complications include wound infection & pleural effusion. The major complications include leakage from bile ducts and various anastomoses; intra-abdominal infections, pneumonia, septicemia & bleeding.
Management of these problems involve insertion of tubes under CT scan guidance to drain infected fluid collections, insertion of tubes to divert bile, heavy antibiotics, endoscopic or radiological intervention guided control of bleeding, nutritional support, ICU monitoring, & care. An attempt is always made to continue oral & enteral feeding whenever possible. Rarely a second surgery is required for intra-abdominal infections. It is important to remember that rate of complications is always more in patients with biliary stents due to resistant infections. Although these complications can be dealt with, about 5% of patients will not be able to leave hospital. Thus the success rate is about 95% but is better in younger, fitter patients. Thus selecting patients for resection is very important.
What Will Be The Expense?
The expenses depend upon the hospital where it is done, the concerned consultant & operating team, stay, whether there are postoperative complications, medications required and many more things. Hence it is possible to give an idea about an uneventful surgery, which you should discuss with your consultant in person. Still it will suffice to say that it involves significant expense.
Will I Need Chemotherapy?
It is now standard treatment to give chemotherapy once you recover from the resection surgery. This is called adjuvant chemotherapy. Chemotherapy is also given if the final histopathological report shows incomplete removal in spite of an apparently successful surgery. This can happen in a small percentage of patients.
How Long Will It Go On?
Chemotherapy will only be started once you have fully recovered from your operation and have gotten over any post-operative complications. Usually six treatments (or cycles) are given by a local medical oncologist (cancer doctor). This period of treatment usually last six months.
Will I Tolerate Chemotherapy?
Immediately after your surgery you will feel quite weak. Even if you are feeling ‘rough’ you can still have the adjuvant chemotherapy and it will not interfere with your rate of recovery. We use adjuvant chemotherapy because it prolongs survival. In particular it is important to appreciate that modern chemotherapy is usually not associated with major side effects.
What Is The Follow Up Schedule After A Successful Surgery?
You will be asked to follow up once in three months with fresh reports of liver function tests, CA19.9 & ultrasonography of abdomen. If the reports show any abnormality then a CT scan of abdomen will be asked. If the reports are normal, three monthly follow up continues for 2 years. A CT scan is performed once a year during these 2 years. After 2 years the follow up is reduced to once in 6 months for next 3 years. In case of doubt a PET CT is done. If a recurrence is suspected then repeat chemotherapy would be given.
What Treatment Can Be Given If A Patient Cannot Be Operated Or Is Beyond Cure On Initial Assessment?
This is called PALLIATIVE TREATMENT. If surgical removal of the cancer is not possible there are many treatments that will be given to help a patient.
BILIARY STENTING
If cancer in the gall bladder is causing a blockage in the bile duct it may be require drainage to relieve jaundice. This may be needed in an otherwise operable patient prior to surgery or a patient who cannot undergo surgery due to advanced age, medical problems or advanced disease. The jaundice can be relieved by inserting a tube (stent) through the tumor during ERCP. If it is not possible to do this by ERCP, then an alternative is by PTHC or a combination of ERCP and PTHC and is called a combined procedure or rendezvous procedure. The stent is about 5–10cm long, made of plastic or self expandable metal and is as thick as a ballpoint pen refill. The stent clears a passage through the bile duct to allow the bile to drain away into the intestine.
When it is done endoscopically , the preparation and procedure is the same as for an ERCP. By looking at the x-ray image the doctor will be able to see the narrowing in the bile duct. The narrowing can be stretched using inflatable balloons (dilators), and the stent can be inserted through the endoscope to enable the bile to drain. Sometimes one may need to put more than one stent to drain all the obstructed ducts. At times the result cannot be achieved by endoscopy and one may have to try percutaneously or as a combined effort (rendezvous). The percutaneous procedure sometimes requires 2 stages. In the 1st , only a drainage catheter is inserted and drains bile outside (external drainage), in the next stage done 4-5 days later the stent is internalized. The metal stent is usually inserted in one stage.
A metallic stent, which is a permanent fixture is better than a plastic stent as it doesn’t get blocked easily. But it is expensive. The plastic stent usually needs to be replaced every 3–4 months to prevent it from becoming blocked. If it does block, you may become jaundiced and have high temperatures. It’s important to tell your specialist about these symptoms as early as possible. You may need antibiotics, and your specialist might advise that the stent be exchanged for a new one. For most people this procedure can be done quite easily.
Stenting should be done only if patient is having symptoms due to jaundice like severe itching. Stenting is not without complications because stent can get blocked and can cause infection and severe sepsis. At times a repeat stenting will be required.
Chemotherapy
This is also advised for patients with a cancer that cannot be removed as this makes you feel better (doctors say ‘improves symptoms’) as well as increasing the length of time that you have to live. Because doctors have still to work out the best type of chemotherapy there are many clinical trials that compare the best available treatment with a new treatment. We have a trial because we do not know if the new treatment is actually better. Patients usually benefit by being in a trial so patients are recommended to consider joining an approved trial. Else one opts for a reasonably proven & efficacious protocol.
Photodynamic Therapy (PDT)
PDT uses a combination of laser light and a light- sensitive drug to destroy cancer cells. A light- sensitive drug is injected into a vein. It circulates in the bloodstream and enters cells throughout the body. The drug enters more cancer cells than healthy cells. It doesn’t do anything until it is exposed to laser light of a particular wavelength.
About two days after the injection you have an endoscopy. The doctor uses an endoscopy tube, like the one used in an ERCP, to shine the laser light on to the cancer. This activates the drug and destroys the cancer cells.
You may be sensitive to light for a few days after the injection. You’ll be told what precautions you need to take until this effect wears off. Other possible side effects include pain, inflammation and nausea. PDT is available in very few centres and is only used as palliative measure .
What Is Done For An Incidentally Detected Cancer After Cholecystectomy For Gall Stones?
This is a fairly common situation and actually is more frequent after the advent of laparoscopic cholecystectomy. If you or your patient has been diagnosed with such a cancer after cholecystectomy, you should visit a specialized hepatobiliary surgeon as soon as possible. He/she will assess you clinically and will get the entire cancer workup done to assess the stage.
Many lucky patients have still localized disease especially if they have come within a short time after the primary surgery preferably within days to a couple of weeks. Patients who come after 3 months often have already widespread disease.
You should carry all the preoperative reports, the operative notes of previous surgeon, the histopathology report. Some details may have to be obtained from your previous surgeon.
Patients with localized disease are advised to undergo a revision surgery involving removal of part of liver near the gall bladder (called gall bladder bed), the nearby lymph glands, sometimes the entire bile duct and the laparoscopy port sites. These patients would invariably be put on chemotherapy later.
Surgery can’t cure gallbladder cancer that has spread beyond the gallbladder. Instead, doctors use radiotherapy or chemotherapy to relieve signs and symptoms of cancer and make you as comfortable as possible.
Above information will help you to make an informed decision but it cannot replace the professional advice and expertise of a doctor who is familiar with your condition. You may have questions that are not covered; you should discuss these with your surgeon. You must remember every individual is different.
Doctors Dealing With Gall Bladder Cancer That You May Meet
Endoscopist: This may be a gastroenterologist or a surgeon who is able to undertake endoscopy (examination of the stomach or bowel using a flexible telescope). A few endoscopists can also perform ERCP and EUS, which are special forms of endoscopy that examine the biliary and pancreatic ducts and the pancreas
Gastroenterologist: A physician who is highly specialised in ‘gut’ problems.
General physician: A consultant medical doctor who works in a hospital and who is broadly specialised including ‘gut’ problems.
General surgeon: A consultant surgeon who works in a hospital and who is broadly specialised including ‘gut’ problems.
HepatoPancreatoBiliary surgeon: A surgeon who is highly specialized in pancreato-biliary & liver operations.
Oncologist: A physician who specializes in chemotherapy for cancer patients.
Glossary
MRI — Magnetic Resonance Imaging Atype of scanning performed to diagnose problems not picked up by regular investigations
CT SCAN – Computerized Tomography
Atype of scanning performed to diagnose problems not picked up by regular investigations
ERCP – Endoscopic Retrograde Cholangiography.
An endoscopic procedure performed to visualize bile & pancreatic ducts & treat the disease endoscopically whenever possible
EUS — Endoscopic UltraSound.
An endoscopic procedure performed to visualize pancreas & biliary tract from very close, diagnose problems, obtain biopsies and at times treat the disease too.
MRCP – Magnetic Resonance Cholangio- Pancreatography
A special type of MRI performed to visualize bile & pancreatic ducts.
Leave a Reply